











































Planning and Implementing a Targeted Polio Vaccination Campaign for Somali Mobile Populations in Northeastern Kenya based on Migration and Settlement Patterns
Centers for Disease Control and Prevention (Harvey, Ward, Merrill, Hsu); International Organization for Migration (Dalal, Amin); Agency for Toxic Substance and Disease Registry, or ATSDR (McIntyre); Task Force for Global Health (Mohamed)
"This project serves as an example for how community-based data collectors and local knowledge can help adapt public health programming to the local context and could aid disease eradication in at-risk populations."
An estimated 3 million ethnic Somalis live in Kenya, predominantly in the Northeastern Region, with lower vaccination coverage reported than any other minority population in the country. The movement and temporary settlement of under-vaccinated mobile Somali populations near and among under-vaccinated ethnic Somali communities in Kenya creates a situation where transmission of poliovirus among children is highly likely. Considering these risks, this project conducted a polio vaccination campaign reaching ethnic Somali children living in mobile populations under the age of 5 years in Garissa County, Kenya. In addition, the project provided measles vaccinations, vitamin A, albendazole, and nutritional support. By outlining the experience of planning and conducting the campaign, this paper provides an example of using community-based data collectors and local knowledge to adapt public health programming to the local context.
The International Organization of Migration (IOM) selected data collectors from the region for their language capabilities (able to speak English, Kiswahili and local Somali dialects) and familiarity with community and local leaders. Twenty facilitators and note-takers were trained in qualitative and geospatial data collection methods and split into four sub-regional collection teams. They also conducted a series of focus group discussions (FGDs) and participatory mapping exercises in order to better understand temporary settlement habits, migration patterns, and health-seeking behaviours. FGDs included community members available at the time of data collection but also individuals identified from the following subgroups: community youth, women, religious leaders, market vendors, healthcare providers and settlement leaders. Facilitators divided focus groups by gender due to cultural sensitivity and to support open dialogue.
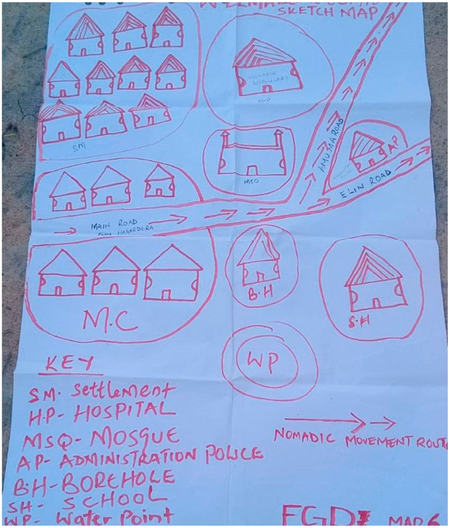
During the FGDs, facilitators posed four main questions with 18 probing questions, designed to assure participants spoke to the key aspects needed for planning a successful campaign. Six of the probing questions called for participants to annotate points of reference on maps. Facilitators used the maps throughout the discussion and asked participants to draw points of interest, a technique known as participatory mapping, to encourage more thorough conversations about migration and settlement patterns, as well as to better understand local spatial knowledge of the region.
Qualitative and geospatial data indicated movement patterns that followed partially definable routes and temporary settlement patterns, with an influx of ethnic Somali migrants (mostly self-identifying as pastoralists) into Kenya at the start of the long rainy season (April-June). Community members also reported that people do not frequent certain health centres that are perceived to lack quality healthcare services, and some health centres refer clients to certain facilities based on their nationality. These factors could be a contributing factor to why unvaccinated children were found during the campaign, as they may not be seeking immunisation or health care services in the region due to distrust or uncertainty of resource availability.
IOM and American Refugee Committee (ARC) implemented an 8-week vaccination campaign at the start of the rainy season (April-May 2019) in Garissa County, Kenya, based on data collected from the FGDs and mapping. Because of ARC's experience working in security-compromised areas, IOM worked jointly with ARC in the vaccination activities through engagements with local authorities, ministry of health, and other implementing actors. In the course of the campaign, 2,196 children aged 0-59 months received polio vaccine (9% had not previously received polio vaccine), 2,524 children aged 9-59 months received measles vaccine (27% had not previously received measles vaccine), 113 were referred for the treatment of severe acute malnourishment, 150 were referred to a supplementary feeding programme due to moderate acute malnourishment, 1,636 children aged 12-59 months were provided with albendazole (for treatment of intestinal parasites), and 2,008 children aged 6-59 months were provided with vitamin A (which improves measles vaccination response).
Thus, this project used local knowledge of settlement and migration patterns to reach those Somali mobile populations frequently missed by vaccination services. FGD data and collaborative relationships with regional facilities allowed for several key vaccination campaign strategies to be followed - for instance, community mobilisers and other leaders provided mass awareness sessions. In addition, IOM and ARC engaged with Garissa County's Department of Health to ensure that the vaccination activities complemented government's immunisation service delivery and supplementary immunisation activities in the region. The campaign had static teams placed at major crossing routes and border villages with little to no access to healthcare, and mobile teams were leveraged to focus on nomadic pastoralist settlements and major water points.
One challenge frequently experienced in delivering immunisation services to mobile populations is the inability to map the locations and movement patterns. This is particularly true in the region of study, as many of the smaller settlements in Northeastern Kenya are not in known geographic information system (GIS) databases. By using local knowledge, the researchers were able to map the general movement patterns and temporary settlement locations of mobile populations in the region. Also, the community-level maps allowed them to use satellite imagery to identify some locations based on hand-drawn key geographical features such as lakes or road intersections, without known global positioning system (GPS) coordinates. A solution to possible mapping errors would be that future campaign planning should work with local populations in several iterations of participatory mapping to create the most accurate depictions of the region to inform public health interventions.
Despite the limitation of not being able to define if the children reached by the campaign were from mobile populations, the researchers believe that the vaccination campaign reached ethnic Somali children and likely migrant Somali children as well. For instance, all chiefs who approved the vaccination campaign in their settlement areas were ethnic Somali, and the area is defined as an ethnic Somali region.
The researchers write: "when working toward international public health goals, such as polio eradication, we recommend that ethnic sub-populations be properly tracked and included in public health figures wherever they reside, regardless of their national identity. Additionally, regional teams should coordinate and communicate across borders as various factors, such as drought and conflict, affect the movement of populations from one area to another....In conclusion, this project exemplified the importance and benefits of collaboration between community-based data collectors and utilization of local knowledge to support outreach of public health interventions....Such methods could therefore be used in future projects to help improve other public health interventions."
Ethnicity & Health. 2022 May;27(4):817-32. doi: 10.1080/13557858.2020.1838455.
- Log in to post comments