












































Rohingya Response: Health Behaviours & COVID-19
"[I]f the perceptions and opinions of Rohingya on healthcare are not taken properly into account and if community awareness and engagement are not prioritized as a key pillar of the COVID-19 response, lessons indicate that the capacity of response actors to control the outbreak will be severely hindered."
Due to factors such as high population density, poor hygiene, insufficient health facilities, and inability to self-isolate, the 855,000 Rohingya refugees residing in 34 camps in Cox's Bazar, Bangladesh are highly vulnerable to COVID-19. Lessons learned from previous epidemic responses, such as Ebola, highlight the role perceptions have on health seeking behaviour, trust in humanitarian responders, and the willingness of affected communities to comply with public health measures. The purpose of this thematic report from ACAPS is to support humanitarian agencies - who, along with the Government of Bangladesh (GoB), began rapidly implementing preventative measures and preparedness and response planning in anticipation of a potential COVID-19 outbreak in the Rohingya refugee camps.
Perceptions included in report have been collected by the International Organization for Migration (IOM)'s Communicating with Communities (CwC) team, which includes Rohingya field researchers, who have been conducting weekly awareness and data collection exercises since March 15 2020. This process has led to these regularly published and/or updated resources:
- COVID-19 Explained: Overview of Rohingya Perceptions and COVID-19 Explained: Essentially Abandoned: Essential Service Restrictions Go into Effect, which are the first 2 of the weekly bulletins intending to provide decision makers with an understanding of the current perceptions, understanding, and information being circulated about COVID-19 among Rohingya within the camps and to inform programming decisions related to a potential outbreak; and
- Flying News about Corona Virus Bulletin, published on March 18 2020.
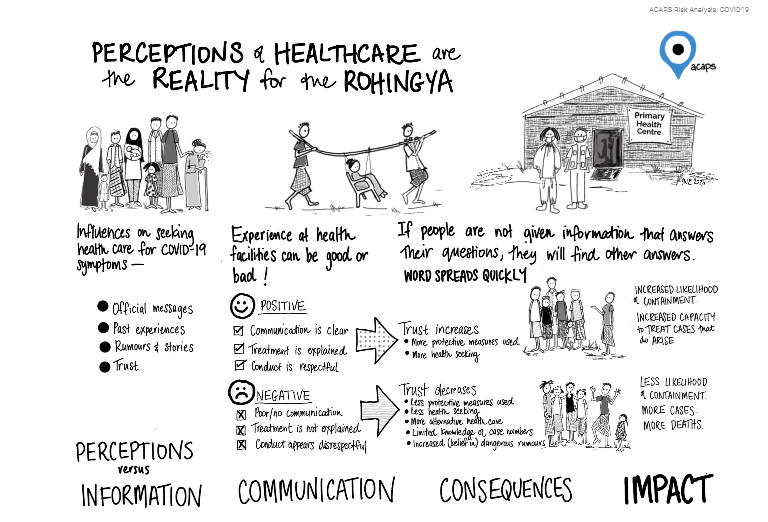
As noted here: "The perception that the Rohingya have of the health system in the camps is their reality and is highly informed by their culture, history, and their understanding of sickness and health." IOM and ACAPS have found that distrust and lack of confidence in the medical system of the response is widespread and is already impacting COVID-19 preparedness efforts. Four main factors contribute to their lack of trust:
- Overloaded healthcare system in camps - There are, of this writing, 154 basic health units, 41 health centres (open 24/7), and 5 hospitals offering free services across the 34 camps. However, the Joint Response Plan for 2020 indicates that these health facilities are unable to meet current caseloads. As a result, patients who go to the camp health facility are often referred to government hospitals and private clinics. The inadequacy of health services is even more prominent for individuals with mobility challenges, such as those with a physical disability, chronic illness, and the elderly, who may face access challenges arising from discrimination and exclusion, as well as inaccessibility in a terrain with steep hills.
- Confidence in alternative healthcare services - Perhaps because of some of the issues cited above, response-wide quantitative or qualitative studies conducted to date confirm that Rohingya households prefer paid health services, available outside of the camps, and will take on debt in order to access it.
- Poor communication and accountability between health staff and patients - For example, a lack of communication between healthcare professionals and patients regarding what is being prescribed, and why, seems to be fueling perception of inadequate treatment. Rohingya have complained about lack of explanation provided and difficulty understanding medical staff. This is, in part, a language issue: The majority of communication in the camps is conducted in Bangla or Chittagonian dialect, yet Translators Without Borders (TWB) found that 36% of refugees have difficulty understanding basic Chittagonian. Rohingya also frequently report feeling disrespected by health workers in the camp facilities: "We are not happy with the hospital because they are busy with their phones and talking together, so we have to wait for a long time and after that they give us only paracetamol, no matter what the disease."
- Experiences from Myanmar - For example, a Rohingya field researcher for IOM's CwC unit explained that the referral system is not common in Myanmar, where people go directly to the doctor who specialises in the illness they have. Visiting a single doctor for all illnesses, only to be referred to another doctor, may explain households' inclination to interpret this as health clinics' inability to provide adequate health care on site.
Major concerns in the context of lessons learned from Ebola (West Africa, 2014-16) already identified in Cox's Bazar include:
- Filling information gaps with rumours and experiences from social connections is already fuelling panic and sowing distrust in advised containment measures - e.g., a particularly harmful and persistent rumour is that health services are killing patients suspected to have contracted COVID-19. This was mentioned in 15 consultations in 9 separate camps.
- COVID-19 preparedness measures, response plans, and their impact on camp health services are unfamiliar to Rohingya and have led to confusion and tension - e.g., one focus group discussion (FGD) participant said, "We went to a health clinic and the health post staff were yelling rudely at Rohingya to stay out of the health post because if we are sick we will spread the illness among us. This is causing panic and stigma."
- Changes in the camps are already reportedly impacting non-COVID-19-related health seeking behaviour and access to services - e.g., FDG participants reported being turned away at health clinics for treatment of non-COVID-19 related illness or symptoms.
- Due to a lack of understanding and familiarity with proposed isolation measures, initial data from 12 FGDs across 7 camps suggests Rohingya are unlikely to comply with those measures - e.g., one female FGD participant said, "We need to get information about isolation, where is it and who will take to go to isolation or take proper care of us. We need to know."
Key lessons to be applied from Ebola:
- Clear, honest, and targeted messaging and engagement of the affected community is needed to build understanding and combat harmful rumours - Research on the Ebola response found that insufficient official information regarding containment, treatment, and expectations of the disease, as well as measures to combat it, meant affected communities based their beliefs on the experiences of others and filled the gaps in their understanding with the scant information available. This reportedly contributed to the rumour in some locations that the vaccine was designed to eradicate a particular ethnic group.
- Positive patient-provider interactions play a critical role, as behaviour of health workers can reinforce negative perceptions, reducing health seeking behaviour and compliance with preventative measures - Ebola-related research indicates that improved interpersonal communication skills of health workers are critical in fostering trust in the healthcare system. In addition, developing patient-provider feedback mechanisms and communication tools that promote positive experiences of community members who directly interacted with healthcare systems could improve perceptions and promote or resort trust in the health system.
- It is necessary to help people gain familiarity with key facilities required to treat the virus in order to ensure trust in them - For instance, during Ebola, a fear of ambulances, because often sick people who went away in them did not return, was found to be a major contributing factor to many not seeking immediate health support when required. In response, responders in Port Loko and Kambia, Sierra Leone held "ambulance exhibitions" that allowed members of the community, including leaders, to inspect the ambulances and judge for themselves that they were safe, clean, and operated by professionals whose main role is to save lives. This successful community engagement strategy was recommended to be applied in other key healthcare facilities, such as clinics and isolation facilities.
Recommendations for COVID-19 response:
- Prioritise proactive measures to pre-emptively address fears and misperceptions that can negatively impact COVID-19 control and response efforts.
- Mobilise Rohingya themselves to engage proactively in the design and implementation of risk mitigation and risk communication activities - This type of bottom-up communication can alleviate mistrust and improve community knowledge and perception of COVID-19; one-way messaging is insufficient to ensure behaviour change.
- Capitalise on positive health seeking behaviour by ensuring those who attend health facilities have positive experiences - This will begin to change the narrative regarding camp health care among the Rohingya.
- Increase transparency and accountability at health facilities from the bottom up by engaging Rohingya community leaders and other community representatives in the monitoring of these services - This may give Rohingya agency to contribute to improvement of these services in ways that also consider their social, cultural, and religious practices.
ACAPS website, April 7 2020; and email from Ana Escaso to The Communication Initiative on June 29 2020.
- Log in to post comments