











































Use of Cellular Phone Contacts to Increase Return Rates for Immunization Services in Kenya
United States Agency for International Development (USAID)'s Maternal and Child Survival Program (MCSP)/John Snow, Inc., or JSI (Mokaya, Mugoya, Shimp); Kisumu County Health Team/Ministry of Health (Raburu)
"Through calling, the health worker is able to establish a personal relationship with the caregivers, understand the reasons behind missing the due date and negotiate with the caregivers on the most appropriate time and date to vaccinate the child."
To address the defaulting of clients who already accessed vaccination services, this operations research in 3 selected districts in western Kenya tested the use of phone call reminders of return dates for caregivers who had brought their children for their first vaccines. In Kenya, failure to complete immunisation schedules by children who previously accessed immunisation services is an obstacle to ensuring they are fully immunised - that is, to complete the vaccination schedule (at birth, 6 weeks, 10 weeks, 14 weeks, 9 months, and 18 months). Yet home visit approaches used to track defaulting children have not been successful in reducing the drop-out rate.
The authors explain that, despite significant progress in the 1980s in reducing the incidence of the 6 most common causes of childhood mortality (tuberculosis (TB), diphtheria, pertussis, tetanus, polio, and measles), coverage levelled off or declined in Kenya. Gains that occurred between 2000 and 2006 were compromised due to issues such as the 2007-08 political conflicts and the proliferation of districts with no clear capacity-building plans for new immunisation managers. Kenya's Health Information System (HIS) reports from 2008 and 2013 indicate that fully immunised coverage had stagnated at 80%, with some districts as low as 30%. Previous studies conducted in Kenya have reported varied reasons for this underperformance, including poor health-seeking behaviour or lack of knowledge of caregivers, inadequate demand generation activities, stock-outs and related logistical problems, inadequate access to hard-to-reach areas, poor defaulter tracing, and/or inadequately trained staff, coupled with irregular supportive supervision.
Part of the issue, and impetus for the study, is that community health workers in Kenya are not paid employees and may be reluctant to perform defaulter tracking activities. Home visits are challenging and may involve the community health workers or public health technicians walking long distances (especially in rural areas) only to find that the client is not at home. Thus, the person would be required to visit the house more than once. This study was therefore developed to determine if a cheaper and more convenient alternative was possible, such as using mobile technology.
Given that household ownership and use of cellular phones in Kenya is reported here to be more than 65%, the researchers surmised that there is potential for using phones to trace defaulters and to increase return rates for immunisation. In Kenya, data capture and management at the facility level are still paper based. A permanent register with details of the vaccinated children is maintained in all immunising health facilities. Although detailed, this permanent register does not raise an alert whenever a child defaults, and the process of generating a manual defaulter list is tedious and time-consuming. To address this challenge, this study introduced a diary (tickler system) with minimum details (name, village, vaccines due, telephone number, name of community health volunteer responsible for child, vaccination status) that could facilitate prompt identification and daily listing of defaulting, thereby aiding effective follow-up of the children by health workers.
Twelve health facilities with high drop-out rates were purposively selected in 4 districts to participate in the study, which involved a longitudinal pre- and post-test design with both quantitative and qualitative arms:
- The quantitative component of the study entailed: registering in a diary children coming for their first vaccines, recording phone contact information of caregivers (or a relative or neighbour, if the caregiver did not have a phone), booking the child for the next visit, and recording the name of the community health worker responsible for the child's residence. If the child did not come for the next appointment, health workers would wait for 2 weeks before calling the caregiver to remind him or her of the missed appointment date.
- The qualitative component entailed asking caregivers who had missed the appointment date to give reasons (self-reported with necessary probing) for not honouring the return date.
In the 12 health facilities, a total of 5,908 children were enrolled and followed up for a period of 9 months, from May 2013 to March 2014. In all of the facilities, caregiver phone ownership was above 80%. A total of 785 defaulters were tracked using the provided phone contacts, whereas 141 were tracked by community health workers or other home visit approaches. Children tracked by the community health workers included those whose caregivers did not provide a phone number or gave incorrect numbers. On average, 1.5 calls lasting 2 minutes (costing Ksh 6, or US$ 0.07) had to be made before the child's status was established and/or the child was brought back to the facility for vaccination services.
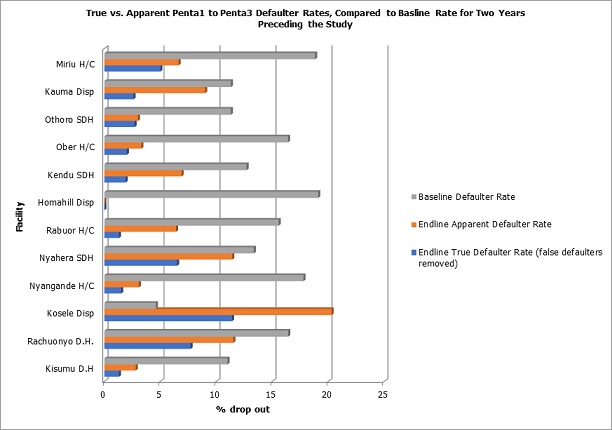
The researchers found that, in 11 of the 12 facilities, defaulter rates between pentavalent1 and pentavalent3 vaccination doses reduced significantly to within the acceptable level of < 10% (see Figure 2). The reluctance to share contact information, especially when the number did not belong to the caregiver, was an initial setback. To mitigate this, training was provided on how to communicate/ask for contact information and to reassure the caregivers that the number would not be shared with unauthorised persons or used for anything unwarranted. Thus, most caregivers provided reliable contact information, and health workers positively perceived phone-based defaulter communications.
In terms of the qualitative findings, the 4 most commonly cited reasons for defaulting immunisation were: competing tasks (especially attending funerals and other social events); fear that the health workers will rebuke them for skipping the return dates; the child was sick; or the child was vaccinated in another facility within or outside the district. (These so-called "false defaulters", unless tracked and documented, contribute to incorrectly elevated defaulter rates.) The pain and excessive crying following the pentavalent vaccination seem to also discourage some caregivers from bringing a child back to complete the schedule. Additional communications are needed to address this, say the researchers. Traditional beliefs did not feature strongly as a reason for defaulting immunisation services.
The researchers explain that, in the first two months of the study, some caregivers delayed coming for their appointment until they received the call from the health workers. In order to address this problem, health workers from the facility and the community health workers participating in the study were encouraged to counsel mothers on the benefits of honouring the appointment date and vaccinating children in a timely manner. Few caregivers in this study mentioned "forgetting the return date" as a reason for not honouring the return date. However, the assumption that caregivers forget appointment dates has triggered the development and implementation of several SMS (short messaging service, or text)-based reminder platforms in various parts of the world. Considering this study's findings, reminder SMS messages alone may not resolve the lack of continuity of participation in immunisation services. An SMS does not provide the health worker with the opportunity to get proper feedback from the client. Although calling is perceived to be expensive, this study provides evidence that the cost of implementing the call approach is feasible - and more effective than texting caregivers alone.
It was found that caregivers who provided phone contact information for their male spouses were more likely to respond to calls favourably and have their children vaccinated, which could reflect the decision-making power vested in male spouses in western Kenya. This finding needs further analysis, the researchers assert, as children were not brought to the clinic by their fathers, nor were females accompanied by their spouses. This implies low male involvement in the child's vaccination session: "To also improve participation in immunization, additional communication activities to encourage male involvement are potentially important for health programs to consider."
"As a result of this study, county managers in the intervention counties have been encouraged by the Kenya immunization program to incorporate this low-cost defaulter tracking mechanism as part of their service delivery and client interactions, along with the use of community resource persons. In addition, as approximately 40% of the defaulters in the intervention facilities were not real defaulters (i.e. the children were vaccinated elsewhere), it has been recommended that counties develop a[n]...information-sharing system between health facilities...to minimize potential wastage of facility resources on tracking children who are already vaccinated. Monthly facility in-charges meetings or/and the quarterly review meetings provide such a platform for sharing this information."
The Pan African Medical Journal 2017;28:24. DOI: 10.11604/pamj.2017.28.24.12631 - sourced from - Maternal and Child Survival Program (MCSP) website, March 15 2018.
- Log in to post comments