











































Improving Vaccination Uptake among Adolescents
University of Cape Town (Abdullahi, Kagina, Hussey); Stellenbosch University (Ndze, Wiysonge); South African Medical Research Council (Wiysonge)
"[T]his review could be used to advocate for strengthening existing adolescent vaccination policies and to formulate new policies on the vaccination of adolescents where none currently exist."
In recent years, many programmes have been launched to increase the uptake of different vaccines in adolescent populations; however, vaccination coverage among adolescents remains suboptimal. Commonly reported barriers include: lack of knowledge about vaccines and vaccine-preventable diseases (VPDs); negative attitudes towards vaccination from adolescents, parents, teachers, and healthcare providers; poor vaccine infrastructure; and financial constraints. Interventions to address these barriers may have multiple components, reaching out to adolescents and their communities, healthcare providers, the health system, or a combination of these. This Cochrane Review aimed to assess the effects of approaches to increase the number of adolescents who get vaccinated.
In October 2018, the researchers searched 11 databases, 2 clinical trials platforms, electronic databases of grey literature, and reference lists of relevant articles. For related systematic reviews, they searched 4 databases. In May 2019, they performed a citation search of 5 other websites. This led them to include in the review 16 studies (8 individually randomised trials, 4 cluster randomised trials, 3 non-randomised trials, and one controlled before-after study). Twelve studies were conducted in the United States (US), while there was one study each from: Australia, Sweden, Tanzania, and the United Kingdom (UK). The outcomes included uptake of: human papillomavirus (HPV) (11 studies); hepatitis B (3 studies); and a combination of tetanus-diphtheria-acellular-pertussis (Tdap), meningococcal, HPV, and influenza (3 studies) vaccines. Ten studies had unclear or high risk of bias.
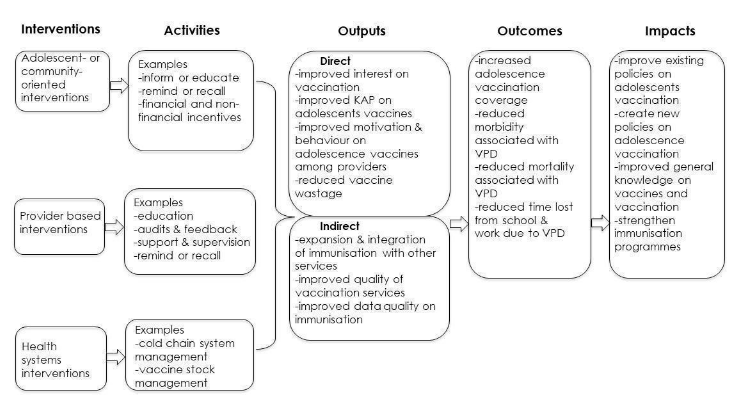
The researchers categorised interventions as:
- Recipient-oriented - including:
- Educational interventions that help adolescents and their communities understand the meaning and relevance of vaccination to their health. Such interventions may be delivered face to face or via written mail, telephone conversation, audiovisual presentation or drama, printed materials, websites, multi-media campaigns, or community events.
- Client reminder interventions delivered using various methods, such as telephone calls, letters, or postcards.
- Adolescent or community incentives that provide financial or other incentives to motivate people to accept vaccinations.
- Mandatory vaccination, which refers to a law or policy that requires students to show proof of immunisation records prior to school admission.
- Provider-oriented - including:
- Provider reminder interventions informing vaccinators that individual clients are due for vaccinations, delivered through client charts, computer, email, or postal mail, among others.
- Audit and feedback for vaccinators that involves retrospectively evaluating the performance of the vaccinators in administering vaccines and providing feedback, so as to motivate providers to improve immunisation services.
- Provider education that seeks to increase provides' knowledge and to encourage them to adopt positive attitudes towards vaccination. Techniques by which information is delivered can include written materials, videos, lectures, continuing medical education programmes, and computerised software.
- Health-systems-oriented, such as carrying out outreach programmes (school-based immunisation and mass campaigns), expanding access in healthcare settings, and reducing out-of-pocket costs.
Key findings:
- Health education improves HPV vaccine uptake compared to usual practice (relative risk (RR) 1.43, 95% confidence interval (CI) 1.16 to 1.76; 3 studies, 1,054 participants; high-certainty evidence). In addition, one large study provided evidence that a complex multi-component health education intervention probably results in little to no difference in hepatitis B vaccine uptake compared to simplified information leaflets on the vaccine (RR 0.98, 95% CI 0.97 to 0.99; 17,411 participants; moderate-certainty evidence).
- Financial incentives may improve HPV vaccine uptake compared to usual practice (RR 1.45, 95% CI 1.05 to 1.99; 1 study, 500 participants; low-certainty evidence). However, it is unclear whether combining health education and financial incentives has an effect on hepatitis B vaccine uptake, compared to usual practice (RR 1.38, 95% CI 0.96 to 2.00; 1 study, 104 participants; very-low-certainty evidence).
- Mandatory vaccination probably leads to a large increase in hepatitis B vaccine uptake compared to usual practice (RR 3.92, 95% CI 3.65 to 4.20; 1 study, 6,462 participants; moderate-certainty evidence).
- Provider prompts probably make little or no difference compared to usual practice, on completion of Tdap (OR 1.28, 95% CI 0.59 to 2.80; 2 studies, 3,296 participants), meningococcal (odds ratio (OR) 1.09, 95% CI 0.67 to 1.79; 2 studies, 3,219 participants), HPV (OR 0.99, 95% CI 0.55 to 1.81; 2 studies, 859 participants), and influenza (OR 0.91, 95% CI 0.61 to 1.34; 2 studies, 1,439 participants) vaccination schedules (moderate-certainty evidence).
- Provider education with performance feedback may increase the proportion of adolescents who are offered and accept HPV vaccination by clinicians, compared to usual practice. Compared to adolescents visiting non-participating clinicians (in the usual practice group), the adolescents visiting clinicians in the intervention group were more likely to receive the first dose of HPV during preventive visits (5.7 percentage points increase) and during acute visits (0.7 percentage points for the first and 5.6 percentage points for the second doses of HPV) (227 clinicians and more than 200,000 children; low-certainty evidence).
- A class-based school vaccination strategy probably leads to slightly higher HPV vaccine uptake than an age-based school vaccination strategy (RR 1.09, 95% CI 1.06 to 1.13; 1 study, 5,537 participants; moderate-certainty evidence).
- A multi-component provider intervention (including an education session, repeated contacts, individualised feedback, and incentives) probably improves uptake of HPV vaccine compared to usual practice (moderate-certainty evidence).
- A multi-component intervention reaching out to providers and parents involving social marketing and health education may improve HPV vaccine uptake compared to usual practice (RR 1.41, 95% CI 1.25 to 1.59; 1 study, 25,869 participants; low-certainty evidence).
Notably, most of the evidence is of low to moderate certainty. Therefore, additional research is needed to further enhance adolescent immunisation strategies, especially in low- and middle-income countries (LMICs) where there are limited adolescent vaccination programmes. Given that there is little or no evidence from existing studies on cost and (gender, socioeconomic, and geographical) equity, a challenge for the future is to design rigorous evaluations and report results in ways that can assess costs and equity impacts clearly, in addition to vaccination knowledge, intentions, and coverage.
In addition, say the researchers, it is critical to understand the factors that influence hesitancy, acceptance, and demand for adolescent vaccination in different settings. This is the topic of an ongoing Cochrane qualitative evidence synthesis, which may help to explain why and how some interventions were more effective than others in increasing adolescent HPV vaccination coverage.
Cochrane Database of Systematic Reviews. https://doi.org/10.1002/14651858.CD011895.pub2.
- Log in to post comments